Treatment planning is performed on a static CT dataset, capturing a single snapshot. The resulting plan is then delivered to the patient over multiple weeks, relying on efforts to recreate that initial anatomy and setup for every fraction.
Surface Guided Radiation Therapy (SGRT) technologies have become invaluable in helping position patients consistently, using surface metrics to guide alignment. Yet, typical SGRT tolerances — often set generically at 3–5 mm and 3 degrees — are rarely customized to individual patients or specific anatomical sites. These thresholds don’t reflect the actual dosimetric consequences of deviations for a given patient. Patients with limited mobility introduce additional challenges in reproducibility. Even with careful setup, small positional inconsistencies can result in subtle, unintended dose shifts. In some cases, evidence of excessive or misplaced dose to normal tissues is only discovered after treatment has been delivered, when the opportunity to intervene has passed.
Patients, after all, are not phantoms, and Patient Specific Quality Assurance (PSQA) activities lose clinical meaning when a surrogate phantom stands in for the patient for independent secondary calculations and IMRT QA process. After all the checks and approvals are done and a patient is prepared for the start of treatment, their anatomy has already changed, and it continues to change throughout the course of treatment. Breast tissue can swell or develop seromas. Abdominal organs fluctuate with varying gas or solid content. The pelvis undergoes daily shifts with bladder or rectal filling. Even with Image Guided Radiation Therapy (IGRT) to align to internal anatomy and minimize gross setup errors, the insight into how day-to-day anatomical changes impact the actual dose delivered is still lacking. So the question remains:
- How do we adapt and personalize our SGRT and IGRT setup tolerances based on the true dosimetric situation for each patient?
- How does moving to more individualized tolerances help clinicians decide when it’s safe to treat versus when to adapt or replan?
The Challenge Is Recognized — But Not Universally Solved
Unseen dosimetric uncertainty is now acknowledged across the field. Sophisticated platforms like the Elekta Unity MR-linac offer online adaptive radiotherapy workflows such as Adapt to Position (ATP), which aligns the day’s image to the reference via rigid registration and updates the plan accordingly. However, these solutions require significant infrastructure. Many clinics lack such technology, yet still face the same challenges of anatomy-driven dose variability.
Where RadCalc Is Heading
At LAP, we’re addressing this gap by building on our core strengths: precise alignment and independent dose verification. LAP lasers and LUNA 3D offer continuous, non-invasive surface tracking from simulation through delivery. Paired with RadCalc’s 3D QA suite, we’re creating an integrated workflow to make dosimetric insight patient-specific and actionable.
RadCalc’s EPID dosimetry already allows clinics to assess the dose delivered retrospectively. However, proactive insight is needed before or during treatment, not just after.
Redefining QA: Integrated SGRT and Dose Evaluation Workflows
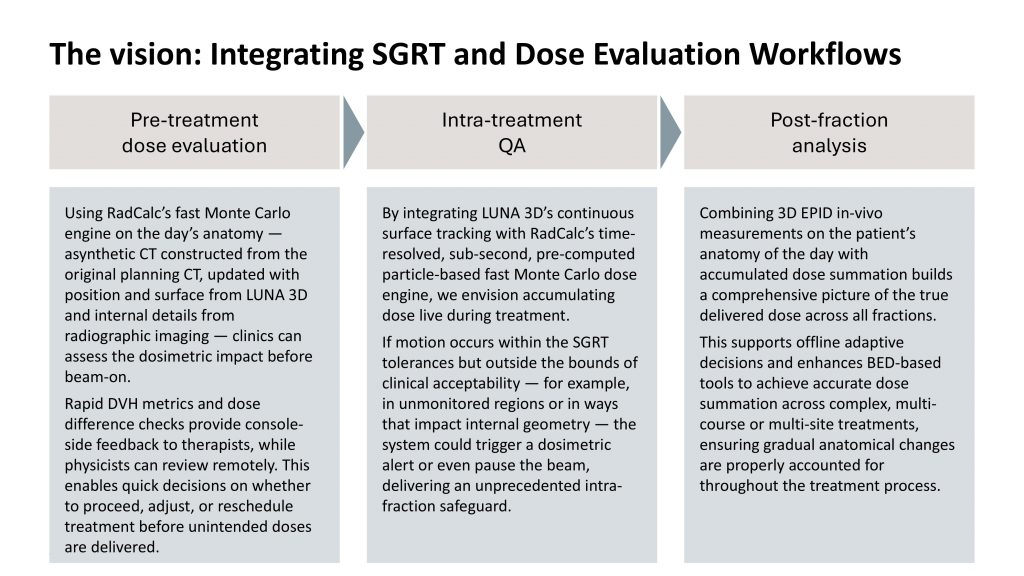
RadCalc’s future centers on combining SGRT and adaptive QA through three key workflows, as shown in the vision presented in Figure 1.
A Smarter, Patient-Centric QA Standard
Together, these tools help clinics move from fixed tolerances to a personalized, dosimetrically grounded approach — no MR-linac required. With RadCalc, QA becomes dynamic, data-driven, and built around the patient, not the plan.
Let’s connect and explore how this evolution in QA can support your clinic’s vision!
Note: German Patent Application No. 10 2023 115 102.9, PCT Patent Application No. EP2024/065566, US Patent Application No. 19/144,366

Carlos Bohorquez, MS, D.A.B.R, is the Product Manager for RadCalc at LifeLine Software, Inc., a part of the LAP Group. An experienced board-certified Clinical Physicist with a proven history of working in the clinic and medical device industry, Carlos’ passion for clinical quality assurance is demonstrated in the research and development of RadCalc into the future.